



Test Blend 400 Genli Pharmaceuticals Best USA
Test Blend 400 Genli Pharmaceuticals is a high-potency injectable testosterone formulation designed for intramuscular use in testosterone replacement therapy (TRT). Each 10 mL vial delivers 400 mg/mL of testosterone through a strategic combination of three esters: testosterone cypionate (187 mg), testosterone enanthate (188 mg), and testosterone propionate (25 mg). This multi-ester profile allows for both immediate and sustained hormonal action, promoting stable serum testosterone levels with fewer injections. Ideal for clinical use in treating male hypogonadism, Test Blend 400 provides a comprehensive androgenic profile with optimized pharmacokinetics.
Test Blend 400 Genli Pharmaceuticals: Comprehensive Medical Review for Testosterone Replacement Therapy
Test Blend 400 Genli Pharmaceuticals – also known as a Test 400 tri-blend testosterone injection – is a high-concentration formulation combining three esterified testosterone variants in one 10 mL vial (400 mg/mL total). It is produced by Genli Pharmaceuticals under the name Super Test 400, containing a mixture of short- and long-acting testosterone esters (Testosterone Propionate, Enanthate, and Cypionate). This comprehensive review examines what Test Blend 400 is, its exact composition, pharmacokinetics (half-life and release profile), recommended dosage and use in TRT cycles, expected results, and importantly the potential side effects and long-term risks. Disclaimer: Testosterone therapy should only be used under medical supervision and according to local laws.
What is Test Blend 400? (Overview and Purpose)
Test Blend 400 is a three-testosterone blend (tri-ester mix) designed for intramuscular injection, primarily aimed at treating male hypogonadism or as part of testosterone replacement therapy (TRT). As the name implies, it provides a total of 400 mg of testosterone per mL by combining multiple esters in one solution. In the case of Genli’s product, each 1 mL contains: 187 mg Testosterone Cypionate, 188 mg Testosterone Enanthate, and 25 mg Testosterone Propionate. This 3-Test 400 blend (10 mL vial, 400 mg/mL) formulation is conceptually similar to other multi-ester testosterone products (for example, Ultima Tri Test 400 blend by another manufacturer), wherein short-, intermediate-, and long-acting esters are combined.
The rationale for such a blend is to achieve both an immediate release of testosterone (from the short propionate ester) and a sustained release over a week or more (from the longer enanthate and cypionate esters). In theory, this could provide a quick onset of action and maintain more stable testosterone levels between injections, potentially reducing injection frequency compared to single-ester formulations. Test Blend 400 is sometimes marketed toward athletes and bodybuilders (hence frequent “Test Blend 400 review” discussions on forums like Reddit) seeking strength and muscle gains, but it is also purported for legitimate TRT use in men with diagnosed low testosterone.
Clinically, however, it’s important to note that while multi-ester formulations (such as the well-known Sustanon 250 blend) were designed to mimic physiologic testosterone release and allow less frequent dosing, real-world pharmacokinetics often differ from the theory. Studies have shown that combining short and long esters can lead to higher initial peaks without significantly prolonging the duration of action, meaning patients may still experience hormonal fluctuations and require frequent injections. In practice, Test Blend 400 is usually injected on a weekly or twice-monthly schedule rather than monthly, similar to single-ester testosterone cypionate or enanthate protocols. This review will delve into the specifics of each component and how they contribute to the blend’s overall effect.
Composition and Ester Breakdown of Test Blend 400 Genli Pharmaceuticals
Test Blend 400 Genli Pharmaceuticals
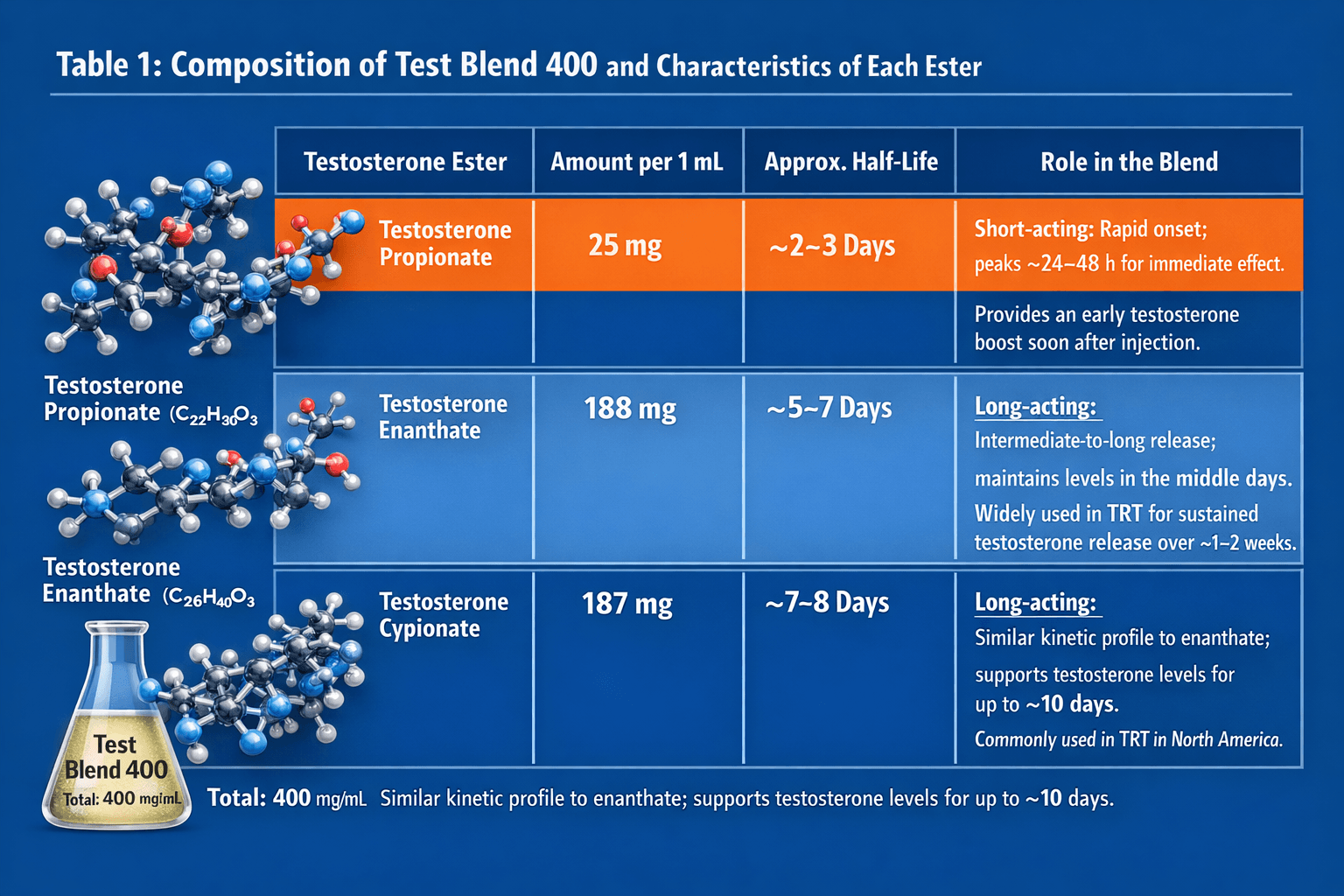
Test Blend 400’s potency comes from its tri-ester composition. Table 1 below summarizes the ingredients per 1 mL and their characteristics:
Table 1: Composition of Test Blend 400 and Characteristics of Each Ester
| Testosterone Ester | Amount per 1 mL | Approx. Half-Life | Role in the Blend |
|---|---|---|---|
| Testosterone Propionate | 25 mg | ~2–3 days | Short-acting: Rapid onset; peaks ~24–48 h for immediate effect. Provides an early testosterone boost soon after injection. |
| Testosterone Enanthate | 188 mg | ~5–7 days | Long-acting: Intermediate-to-long release; maintains levels in the middle days. Widely used in TRT for sustained testosterone release over ~1–2 weeks. |
| Testosterone Cypionate | 187 mg | ~7–8 days | Long-acting: Similar kinetic profile to enanthate; supports testosterone levels for up to ~10 days. Commonly used in TRT in North America. |
All three esters are hydrolyzed in the body to release bioidentical testosterone, which then exerts physiological effects. Differences lie in how quickly they release testosterone into circulation (propionate being fastest, cypionate the slowest). Half-life values are approximate; actual duration of action can vary by individual.
Testosterone Propionate (25 mg) – Fast-Acting Component
Testosterone propionate is a short-chain ester (propionic acid ester) of testosterone. It releases testosterone quickly after intramuscular injection, reaching peak levels within 24–48 hours. Its half-life is roughly 2–3 days, meaning it is largely cleared or inactive after a few days. In the context of Test 400 tri-blend, the 25 mg propionate provides a rapid onset – helping raise serum testosterone soon after the injection. This can be useful for patients to feel quicker symptom relief (e.g. improved energy or libido) at the start of a TRT injection cycle.
However, because of its short action, propionate alone typically requires very frequent administration (every 2–3 days) to maintain stable levels. It is less commonly used by itself in TRT due to the inconvenience of frequent injections and a higher likelihood of injection site pain. Indeed, propionate preparations often cause local irritation or soreness post-injection in some patients, partly due to the ester and the necessary solvents. In Test Blend 400, the low proportion of propionate (only 25 mg out of 400 mg) is intended to mitigate this while still giving an initial “kick.” Clinically, the propionate ester’s role is primarily to boost testosterone levels in the first 1–2 days after administration, bridging the gap until the longer esters take effect.
From a mechanism standpoint, once injected, the lipophilic propionate-testosterone is absorbed fairly rapidly from the muscle depot, then esterases in the bloodstream and tissues cleave the propionate, releasing free testosterone. That free testosterone can then act on androgen receptors or be converted to dihydrotestosterone (DHT) and estradiol, mediating the hormone’s effects. Because propionate is released quickly, it can lead to an early supraphysiologic peak in testosterone levels shortly after injection. This peak can contribute to side effects (e.g. transient mood changes or estrogen spike) if not managed, a point we will revisit when discussing the blend’s pharmacokinetics and side effect profile.
Testosterone Enanthate (188 mg) – Long-Acting Component
Testosterone enanthate is a commonly used long-acting testosterone ester, containing a 7-carbon heptanoate chain. It has an absorption half-life around 5 to 7 days, with some variability (often cited ~4.5–7 days). Enanthate by itself is a mainstay of TRT internationally; for example, it has been in use since the 1950s for treating hypogonadism. In a single-ester regimen, testosterone enanthate is typically injected every 1 to 2 weeks in clinical practice.
In Test Blend 400, the 188 mg of enanthate constitutes nearly half the total content. This provides the sustained release of testosterone after the propionate fades. After intramuscular injection, enanthate is gradually absorbed from the oil depot into circulation over several days. As the ester is cleaved, it maintains elevated testosterone levels roughly from day 2 through day 10 post-injection (overlapping with cypionate’s effect). The product description for Super Test 400 notes that serum levels “remain elevated for 7 to 10 days” after an injection, thanks largely to the enanthate and cypionate content.
Mechanistically, enanthate’s longer half-life is due to its higher lipophilicity and longer carbon chain, causing a slower release from the muscle and slower hydrolysis. Once free testosterone is released, it acts the same as any endogenous testosterone: binding androgen receptors in muscle, bone, fat, and the nervous system, or being converted to DHT (which has potent androgenic effects on skin, prostate, hair follicles) or aromatized to estradiol (affecting bone density, mood, etc.). The clinical relevance of enanthate in TRT is well-established: a standard dose (e.g. 100–200 mg weekly or 200–250 mg biweekly) can reliably raise testosterone into the normal range for hypogonadal men. Enanthate’s inclusion in a blend simply means it should behave as it normally would, contributing a stable mid-term testosterone level.
It’s worth noting that enanthate and cypionate are often considered interchangeable in practice. They have very similar kinetic profiles, as we will discuss next. In some countries, enanthate (e.g. Testoviron Depot) is more widely available, whereas in the U.S. cypionate (Depo-Testosterone) has been the traditional choice. Test Blend 400 containing both is somewhat redundant pharmacologically, but may be a manufacturing choice (possibly to reach the 400 mg concentration by combining esters).
Testosterone Cypionate (187 mg) – Long-Acting Component
Testosterone cypionate is another long-acting ester, nearly identical in behavior to enanthate. Cypionate has an 8-carbon ester (cyclopentylpropionate) and a half-life of roughly 7–8 days. Some sources quote a half-life range of about 8–12 days for cypionate, but in practical terms it’s on the order of a week. Like enanthate, cypionate is typically administered every 1–2 weeks in TRT regimens, and it produces a similar testosterone peak and decay pattern. In fact, as one pharmacology text notes, “Testosterone cypionate shows the same kinetic profile as enanthate.”
In Test Blend 400, 187 mg of cypionate (virtually equal to the enanthate content) serves to prolong the serum testosterone elevation through the latter part of the dosing interval. Its release and action overlap heavily with enanthate’s; together these two esters (total ~375 mg) dominate the blend’s longer-term effect for up to 10+ days. After injection, testosterone cypionate is steadily absorbed from the depot (the product uses an oil carrier, often cottonseed or similar, which influences release rate). By approximately one week post-injection, levels from cypionate (and enanthate) begin to taper, potentially approaching baseline by around 14 days if not re-dosed.
The presence of both cypionate and enanthate in one formulation does not dramatically change the pharmacology – it essentially ensures a high concentration of long-acting testosterone. Clinically, a benefit of using such a high total dose per mL could be reduced injection volume for those needing higher doses. For instance, instead of injecting 2 mL of a 200 mg/mL enanthate solution, a patient could inject 1 mL of a 400 mg/mL blend to receive ~400 mg of testosterone. (However, 400 mg is a supra-physiologic dose for TRT; we will discuss dosing shortly.) The mechanism of action of cypionate is the same as enanthate once hydrolyzed – raising systemic testosterone that then interacts with androgen receptors. Importantly, because cypionate (like enanthate) is long-acting, it can lead to a prolonged suppression of the hypothalamic-pituitary-gonadal axis; exogenous testosterone will feedback inhibit natural testosterone production. This occurs with any ester if the dose is sufficient, and necessitates careful use in TRT (to avoid shutting down fertility without planning, etc.).
In summary, the enanthate and cypionate in Test Blend 400 form the foundation of sustained testosterone release, while propionate provides an initial surge. All esters ultimately yield the same active hormone, so the blend’s uniqueness lies in its pharmacokinetic profile rather than a different pharmacodynamic action.
Pharmacokinetics and Half-Life of Test 400 blend Genli Pharmaceuticals
Pharmacokinetically, Test Blend 400 behaves as a multi-phase testosterone delivery system. After an intramuscular injection of this testosterone blend, serum testosterone concentrations rise rapidly within the first day (due to propionate) and then are sustained for roughly a week or slightly more (due to the enanthate and cypionate). The manufacturer notes an initial spike within 24 hours and an elevated level for 7–10 days post-injection. This suggests that a weekly injection schedule would keep testosterone in an augmented range consistently, whereas going much beyond 10–14 days between injections could allow levels to fall back toward baseline.
To understand “Test 400 blend half-life,” we must consider the contributions of each ester. There is no single half-life for the combined mixture, but effectively the shortest component (propionate) dictates the early clearance and the longer components (enanthate, cypionate) dictate the tail end. The functional half-life of the blend can be thought of as roughly a week (since the bulk is long-ester) – after one week, a significant portion of the testosterone from the dose will have been released and metabolized. By two weeks, levels are likely low enough that another injection is needed to avoid dipping into hypogonadal range.
It’s important to dispel a common misconception: combining esters does not magically produce completely steady hormone levels without peaks and troughs. In fact, clinical pharmacology references emphasize that multi-ester formulations like Sustanon (which contains both short and long esters, similar in concept to Test 400) can cause even higher initial peaks and still eventually drop off, rather than flattening the curve. One expert summary notes that Sustanon’s design to allow 3–4 week dosing intervals “in practice falls short” – patients often experience a spike then a dip, and weekly or twice-weekly injections end up needed to maintain stability. Essentially, the short ester causes a surge, and once it and some medium esters clear in the first week, the remaining long ester alone (decanoate in Sustanon’s case, or enanthate/cypionate in Test 400) may not fully prevent a trough by week’s end. In line with this, Test Blend 400 is generally administered on a 1-week cycle (or sometimes split into two smaller injections per week) to keep levels in a steady therapeutic window.
From a metabolism standpoint, once the testosterone from any ester is in circulation, it is handled like endogenous testosterone: a small fraction remains free, while the majority binds to sex hormone-binding globulin (SHBG) and albumin. The free portion is what’s biologically active, and testosterone’s elimination (through liver metabolism to inactive metabolites excreted in urine) correlates with how much is free vs. bound. The different esters do not change how testosterone is eliminated once it’s free; they only modulate how quickly it enters the bloodstream.
In summary, the half-life of Test Blend 400’s effects is governed primarily by the enanthate and cypionate (~1 week). Patients can expect a rapid peak (perhaps within 1–2 days) and then a gradual decline over 1 to 2 weeks. If used for TRT, most clinicians would likely dose it weekly to avoid end-of-cycle trough symptoms (e.g. fatigue or low mood before the next injection). If dosed every two weeks, there may be a higher swing – very high levels just after injection and potentially sub-therapeutic levels by day 14, especially given propionate and part of enanthate would be gone. This fluctuation can be mitigated by shorter intervals or dividing doses.
Practical note: Patients and providers should be aware that the peak level achieved with a 400 mg dose is quite high; initially, this can be supraphysiologic (above normal range), which might increase side effect risk (e.g. transient high estradiol levels). Monitoring and possibly adjusting the dose can help tailor the pharmacokinetic curve to the individual’s needs. We will later discuss how these kinetics relate to clinical outcomes and side effects (such as the risk of “peaks and valleys” in mood or libido some men report when on longer-interval injections).
Clinical Use of Test Blend 400 Genli Pharmaceuticals: Dosage, Cycles, and Expected Results
Test 400 Genli Pharma Dosage and Administration in TRT
When it comes to dosage, it’s crucial to distinguish between manufacturer recommendations for this high-concentration blend and the dosing principles of evidence-based TRT. Genli Pharmaceuticals’ Super Test 400 literature suggests an adult male dose of 400–600 mg injected IM every 1 to 2 weeks. This dosing range is notably higher than traditional TRT doses, which typically start around 75–100 mg per week for enanthate/cypionate (e.g. 150–200 mg every 2 weeks) to achieve mid-normal testosterone levels. A dose of 400 mg/week, in a medical context, would generally produce supraphysiological testosterone concentrations in most men. Therefore, clinicians would usually titrate the dose based on the patient’s blood levels and symptoms, possibly using much less than 1 mL of Test Blend 400 at a time. For example, 0.25 mL (100 mg) weekly of Test 400 could approximate a standard TRT dose (since 100 mg of a long ester weekly often suffices to bring levels to normal range).
In practice, some TRT clinics or protocols might use 250–400 mg of long-acting testosterone but spread out over longer intervals. For instance, Nebido (testosterone undecanoate) is 1000 mg every 8–12 weeks in some regimens. However, that formulation is specifically designed for very extended release. For Test Blend 400, a more frequent dosing is prudent. A reasonable medical approach might be 200 mg (0.5 mL) weekly, then adjust if trough levels are low or symptoms persist. The goal is to maintain serum testosterone in the mid-normal physiological range (roughly 400–800 ng/dL in many labs) throughout the dosing cycle. Regular monitoring of blood testosterone (measured halfway between injections for trough, or periodically at peak and trough) can guide proper dosing.
For subcutaneous injection: Single-ester testosterone solutions (like cypionate) are sometimes given subcutaneously in smaller volumes with good effect. While intramuscular (IM) is the classic route, Test Blend 400 could theoretically be used subcutaneously if the volume is small (e.g. 0.2–0.5 mL) – but one must be cautious with the high concentration potentially irritating tissue. The manufacturer’s guidance is IM use.
“Cycles” and Athletic Use Considerations
The term “Test Blend 400 cycle” is more commonly encountered in bodybuilding and athletic circles than in medical literature. It refers to using this product in a cycle of anabolic steroid use, typically at higher-than-TRT doses, often combined with other drugs, for a period of weeks to months, followed by a break or post-cycle therapy. While our focus is medical, it is important for clinicians to be aware of this context, as patients may present having used such compounds on their own.
Anecdotally, users on forums (e.g., Test Blend 400 Reddit discussions) report running cycles of 8–12 weeks with weekly doses in the 400–800 mg range, expecting significant muscle mass and strength gains. Indeed, 400 mg of testosterone weekly is an anabolic dose that will raise testosterone levels several-fold above normal, likely resulting in increased lean muscle, weight gain (some from water retention), and enhanced recovery and libido in the short term. Such results, however, come with a trade-off of higher side effect risk (acne, blood pressure rise, estrogenic effects, etc., detailed later) and are not medically sanctioned uses.
From a clinical perspective, any use of Test Blend 400 outside a legitimate TRT dose regimen is essentially supratherapeutic. If a patient admits to using it in this way, medical guidance should focus on harm reduction: monitoring labs, ensuring they don’t have dangerously high hematocrit or liver enzymes, and advising on tapering or post-cycle needs to restore natural function. It must be stressed that non-prescribed use of high-dose testosterone is illegal in many jurisdictions and poses health risks.
Expected Therapeutic Results in Hypogonadal Men
When used appropriately for hypogonadism (TRT), the expected results of Test Blend 400 are comparable to standard testosterone therapies. Benefits are well-documented in medical studies: improved sexual function and libido, increased energy and mood, gains in muscle mass and strength, reduced fat mass, improved bone mineral density, and potentially improved cognition and quality of life. For example, Osterberg et al. (2014) noted that TRT’s benefits – increased libido, energy, bone density, muscle strength, and even cardioprotective effects – have been observed in hypogonadal men. A recent large randomized trial (TRAVERSE, 2023) specifically found that testosterone therapy (using gel to maintain mid-normal levels) significantly improved sexual function (libido, frequency of sexual activity) and reduced symptoms of depression compared to placebo. These improvements contribute greatly to hypogonadal patients’ quality of life.
It’s important to set realistic expectations on timing of results: many symptomatic improvements (libido, vitality) can occur within weeks, while body composition changes (more muscle, less fat) and bone density improvements take several months to over a year of consistent therapy. There is a known “TRT results timeline” often cited: e.g., sexual benefits in 3–6 weeks, mood and energy within 1–2 months, muscle size noticeably by 3–4 months, bone density increases detectable after 6 months or more.
Using Test Blend 400 for TRT should achieve these same outcomes if dosing is properly managed, since ultimately it raises the serum testosterone into the desired range. One potential advantage of the blend could be slightly quicker symptom relief at initiation (due to the propionate’s quick action). For example, a man starting on 200 mg weekly of this blend might feel improvements in libido or mental clarity within days, rather than a couple of weeks, as his levels rise rapidly. The long esters ensure that after a few doses a steady-state is reached, keeping trough levels from falling too low if timed well.
Athletic/High-Dose “Results”
While not an endorsed use, for completeness: if someone uses Test 400 at high doses (say 400–600 mg/week) as an anabolic steroid cycle, the results typically include substantial increases in muscle hypertrophy and strength, especially when combined with resistance training and adequate diet. Testosterone is a powerful anabolic hormone – studies in young men have shown dose-dependent increases in fat-free mass and muscle strength with supraphysiologic doses (e.g. 600 mg/week) compared to placebo. Users often report gaining several kilograms of weight (a mix of muscle and some water/fat) over a 10–12 week cycle. Recovery and performance can improve, and often there is a pronounced increase in training intensity due to enhanced recovery.
However, these “performance” results come with significant risk and are outside the scope of therapeutic TRT. Such usage will shut down the body’s natural testosterone production (requiring post-cycle therapy to restart, if at all), and can predispose the individual to the side effects we describe below. Any patient citing “Test Blend 400 results” from online anecdotes or Reddit should be counseled that anecdotal reports are not scientific evidence. Moreover, the law of diminishing returns and health risks becomes relevant – higher doses yield more side effects disproportionately.
In summary, Test Blend 400 can be an effective form of testosterone for treating deficiency, providing the full spectrum of benefits of TRT when used in appropriate doses. Its unique blend nature does not confer magical gains beyond what standard testosterone enanthate or cypionate would, but it is a potent delivery vehicle. Both patients and providers should ensure dosing is individualized and err on the side of using the minimum effective dose to alleviate symptoms, thereby reducing risk of adverse effects.
Test Blend 400 Genli Pharmaceuticals Potential Side Effects and Long-Term Risks
No testosterone therapy is without side effects. The side effect profile of Test Blend 400 will mirror that of any injectable testosterone, with some considerations due to its high concentration and multi-ester peaks. Side effects can be categorized into estrogenic effects, androgenic effects, polycythemia and cardiovascular risks, metabolic effects, and injection-related issues, among others. Long-term risks need to be considered, especially if therapy is lifelong. Here we detail the key potential adverse effects and complications, along with discussion of their incidence and mitigation.
Estrogenic Side Effects (Gynecomastia, Water Retention)
Because exogenous testosterone can be aromatized to estradiol by the aromatase enzyme, especially when levels are above physiological range, TRT can lead to elevated estrogen levels in some men. This may result in estrogenic side effects such as:
-
Gynecomastia – the development of breast tissue tenderness or enlargement in males. This is usually dose-dependent and related to how high estradiol rises. Men on high-dose testosterone (e.g. anabolic cycles) are at particular risk, but even TRT doses can unmask gynecomastia in susceptible individuals. Clinically significant gynecomastia is not extremely common on properly dosed TRT, but it can occur, and patients should report any breast swelling or pain.
-
Fluid Retention – estrogen can cause the body to retain water and salt. Men might notice mild ankle edema or a bloated feeling. This is usually mild with TRT, but higher doses (like bodybuilding use of 400+ mg weekly) can cause noticeable water weight gain.
-
Increased Body Fat – paradoxically, while TRT generally reduces fat mass in hypogonadal men, in some cases estrogen-related fat deposition (especially chest or lower abdomen) might occur if estradiol is excessive.
To mitigate estrogenic issues, the goal is to keep testosterone in a reasonable range (avoiding huge peaks). Some patients who are “high aromatizers” might require an aromatase inhibitor (AI) medication in addition to TRT, but this is done cautiously as over-suppressing estrogen can harm bone and metabolic health. It’s often preferable to adjust the testosterone dose before adding an AI. Regular monitoring of serum estradiol levels can guide this if symptoms like gynecomastia emerge.
Androgenic Side Effects (Skin, Hair, Prostate)
Testosterone’s androgenic effects can lead to several side effects, especially in tissues sensitive to DHT (dihydrotestosterone, a metabolite of testosterone):
-
Acne and Oily Skin: Increased androgen activity in the skin’s sebaceous glands can cause acne breakouts or simply oilier skin. This is relatively common in the initial months of TRT, reported by many patients. It often manifests on the back, shoulders, or face. Good skin hygiene and, if needed, consultation with a dermatologist (who may recommend topical retinoids or benzoyl peroxide, etc.) can help. Usually the acne is mild to moderate; severe acne is less common but can occur at higher doses.
-
Hair Loss (Androgenic Alopecia): Men genetically predisposed to male pattern baldness may experience accelerated hair thinning on the scalp when on testosterone. This is due to conversion of testosterone to DHT in hair follicles, which can miniaturize follicles. Not every man will have this issue, but those with a family history of baldness might notice faster progression. Management may include DHT-blocking medications like finasteride, although these carry their own side effects and must be used under guidance.
-
Prostate Effects: The prostate is an androgen-sensitive organ. Testosterone (and especially DHT) can stimulate prostate tissue. Benign prostatic hyperplasia (BPH) symptoms (such as increased urinary frequency, urgency, or weak stream) could potentially worsen in men on TRT. However, interestingly, studies have shown mixed results. Short-term TRT tends not to significantly worsen lower urinary tract symptoms in most men, and some reports even suggest no change or slight improvement in urinary symptoms over time. Testosterone does cause a slight increase in prostate volume on average (in one study ~12% increase), but this doesn’t always translate to clinical symptoms. That said, any man with pre-existing BPH should be monitored. If urinary symptoms significantly worsen on TRT, dosage reduction or consultation with a urologist is warranted.
-
Prostate Cancer Risk: Historically, there has been concern that testosterone could “feed” an occult prostate cancer, stemming from the fact that androgen deprivation is a treatment for prostate cancer. Current evidence indicates that TRT does not create de novo prostate cancer in men who didn’t have it, nor does it appear to markedly increase the risk, provided proper screening is done. A famous study by Marks et al. found that 6 months of TRT had little effect on intraprostatic androgen levels or cancer biomarkers in men. More recently, the TRAVERSE trial observed no increase in prostate cancer incidence in men on TRT vs placebo over about two years. However, the standard medical recommendation is: do not give TRT to men with active prostate cancer, and ensure appropriate prostate cancer screening before and during therapy. Guidelines often require a baseline PSA test and periodic PSA monitoring; any significant rise in PSA (e.g. >1 ng/mL within 6–12 months) or abnormal digital rectal exam should prompt evaluation (to rule out previously undetected cancer). In older men, most clinicians will avoid TRT if PSA is above a certain threshold or if there’s high suspicion of prostate malignancy. In summary, TRT should be carefully monitored vis-à-vis prostate health, but when done so, the consensus now is that it is reasonably safe in men without active cancer (some studies even have given TRT to men treated for low-risk prostate cancer without finding high recurrence rates).
Polycythemia and Cardiovascular Risks
One of the hallmark risks of long-term testosterone therapy – especially injectable forms – is polycythemia, or an abnormal increase in red blood cell mass (hematocrit). Testosterone stimulates erythropoiesis (red blood cell production) in the bone marrow, which can be beneficial in men with anemia but problematic if it overshoots. Studies estimate that over 20% of men on TRT develop elevated hematocrit beyond the normal range. This is more common with injectable testosterone (like enanthate/cypionate blends) than with transdermal gels, because injections produce higher peaks that strongly drive erythropoietin and RBC production.
-
Polycythemia (Erythrocytosis): This refers to hematocrit (HCT) levels above the normal limit (often HCT >52–54% is used as a threshold for intervention). Elevated hematocrit increases blood viscosity, which in turn may raise the risk of vascular thromboses – clots that can cause stroke, heart attack, or deep vein thrombosis. While these serious events are theoretical risks (clear causal links in TRT patients are not strongly proven, partly because doctors usually intervene before it gets severe), it is accepted that polycythemia is an adverse effect of TRT that needs managing.
Incidence: A significant fraction of men on injectables get to hematocrit >50%. One study noted >20% incidence as mentioned. Risk factors include higher doses and older age. Test Blend 400, if dosed aggressively, certainly has the potential to cause this effect – one might expect it at least as frequently as with standard testosterone cypionate.
Mitigation: Monitoring of CBC (complete blood count) is mandatory during TRT. Best practice is to check hematocrit at baseline, then 3–6 months into therapy, then periodically (e.g. every 6–12 months). If hematocrit rises above 52% (some guidelines use 54%), the recommendation is often to pause therapy or reduce the dose until it comes down. Therapeutic phlebotomy (periodic blood donation) is another strategy to bring hematocrit down if it creeps up – essentially “bleeding” the patient can relieve the hyperviscosity. In many cases, simply adjusting the dose downward can keep HCT in safe range.
-
Cardiovascular Risks: The relationship between testosterone therapy and cardiovascular risk has been intensely debated. Earlier retrospective studies around 2013–2014 raised alarms about possible increased rates of myocardial infarction and stroke in men (especially older men) on TRT, leading the FDA to mandate a warning about a “possible increased risk of heart attack and stroke” on all testosterone product labels. However, more recent high-quality evidence has been reassuring. The TRAVERSE trial (2023), which was a large placebo-controlled study in men 45–80 (many with cardiovascular risk factors, treated for ~2 years), found no increase in major adverse cardiac events (MACE) in the testosterone group compared to placebo. In fact, there was a very slight (non-significant) reduction in all-cause mortality in the testosterone group and no excess of heart attacks or strokes. This trial has helped ease concerns that TRT, when properly indicated for true hypogonadism, is causing cardiac harm. Observational studies and meta-analyses likewise have not shown a consistent increase in cardiovascular events – some even suggest improvement in certain parameters (like fat loss, insulin sensitivity, which can be cardiometabolic benefits).
That said, one must remain cautious. Men on TRT should be evaluated for cardiovascular risk factors before starting (lipids, blood pressure, etc.) and those with uncontrolled cardiovascular disease should stabilize those conditions first. High-dose usage (steroid abuse) is a different scenario – chronic very high testosterone levels can lead to issues like hypertension, unfavorable cholesterol changes (testosterone can reduce HDL cholesterol), and cardiac muscle changes. There are reports of premature coronary disease and cardiomyopathy in long-term steroid abusers (often using grams of testosterone and other drugs). These outcomes should not be conflated with therapeutic TRT, but they underline that more is not better.
In terms of blood pressure and edema: TRT can cause mild hypertension in some individuals, partly due to water/sodium retention or increased red cell mass. Peripheral edema (swelling of ankles) is listed as a possible side effect and is something to monitor especially in men with heart failure or renal issues.
Bottom line (CV risk): When used in proper doses and with monitoring, testosterone’s benefits often outweigh its risks in hypogonadal men. Recent evidence supports its cardiovascular safety in that context. However, practitioners should monitor hematocrit, blood pressure, and lipid profiles. If hematocrit climbs or if a patient has symptoms like headaches, ruddy complexion, or high blood pressure on TRT, these could be signs of polycythemia and warrant intervention.
Metabolic and Other Effects (Lipids, Liver, Mood, Sleep Apnea)
Testosterone therapy can have various other systemic effects:
-
Cholesterol/Lipid Profile: Exogenous testosterone tends to lower HDL (“good”) cholesterol and can sometimes increase LDL cholesterol. This effect on lipids is generally mild at TRT doses, but is more pronounced at high bodybuilding doses. Over long term, a reduction in HDL could theoretically increase cardiovascular risk, although the clinical significance at TRT levels is unclear. It is wise to re-check lipid panels after starting TRT, and advise heart-healthy lifestyle (diet, exercise) to counter any unfavorable changes. Interestingly, testosterone can also slightly reduce triglycerides and improve insulin sensitivity (some studies have shown TRT reduces diabetes incidence in men with metabolic syndrome). The net effect on cardiovascular health is thus a balance. In one Australian study (T4DM trial), injections of testosterone undecanoate plus lifestyle changes led to a significant reduction in progression to type 2 diabetes in high-risk men – indicating a metabolic positive effect.
-
Liver Function: Unlike oral anabolic steroids (which are 17-alpha-alkylated and can be hepatotoxic), injectable testosterone esters like those in Test Blend 400 do not have direct toxic effects on the liver when used at physiological doses. They bypass first-pass metabolism. Routine liver function tests usually remain normal on TRT. That said, extremely high doses or polypharmacy (using other oral steroids) could affect the liver. There have been rare reports of mild liver enzyme increases or even more serious issues like hepatic adenomas with long-term high-dose steroid abuse, but testosterone by itself in moderate doses is not a major concern for liver injury.
-
Mood and Behavioral Changes: TRT can positively impact mood – many hypogonadal men report improved well-being, confidence, and reduced depression or anxiety on therapy. The TRAVERSE trial explicitly noted improved mood and depression scores with testosterone treatment. However, supraphysiologic levels can in some cases lead to irritability, impulsivity, or aggressive behavior (“roid rage” in colloquial terms). While such extreme mood swings are more commonly associated with very high doses or certain synthetic androgens, clinicians should be mindful of any changes in temperament. Some men might experience increased libido to a degree that it becomes socially problematic or increased energy/restlessness that could manifest as insomnia. These are dose-dependent and can often be managed by dose adjustment. If a patient has underlying bipolar or other psychiatric disorders, careful monitoring is needed as hormone fluctuations can potentially affect those conditions.
-
Fatigue or Sleep Issues: If dosing is not adequate or is too widely spaced, patients might feel a “crash” in energy toward the end of the injection cycle as levels wane. This underscores the importance of optimizing the regimen (possibly more frequent lower doses to avoid peaks and troughs). On the other hand, too high a dose might cause insomnia for some patients. Adjusting timing of injection (e.g., some do better injecting in morning vs evening) could help with sleep.
-
Obstructive Sleep Apnea (OSA): TRT has been associated with worsening of sleep apnea in susceptible individuals. The mechanism isn’t fully clear, but androgens may affect airway patency or respiratory drive during sleep. If a patient has known OSA, they should be cautioned that their apnea could worsen on testosterone; close follow-up or a repeat sleep study might be warranted after starting TRT. For patients who develop symptoms like loud snoring or daytime fatigue on TRT, evaluation for OSA is advised. Some reports note that stopping TRT can alleviate the exacerbation of apnea. Therefore, this is a relative contraindication or caution – not an absolute bar to treatment, but something to manage (e.g., ensuring they use CPAP if they have OSA, and monitoring symptoms).
-
Fertility and Testicular Atrophy: Exogenous testosterone will suppress pituitary gonadotropin (LH/FSH) secretion via negative feedback, leading to reduced intratesticular testosterone, which in turn causes diminished spermatogenesis. Men on TRT often experience a reduction in sperm count and testicular volume (the testes may shrink to some degree due to inactivity). This effect can be significant: studies show TRT can cause azoospermia (zero sperm count) in a substantial portion of men, which is why testosterone was even researched as a male contraceptive. Fertility usually recovers after stopping therapy, but not always immediately; it can take months to a year to regain normal counts, and in a small subset of men, fertility may remain impaired even after cessation (one study found ~10% of men did not recover sperm production after long-term TRT). For a man who may want to father children, this is a crucial consideration. Mitigation strategies include the use of hCG (human chorionic gonadotropin) injections to stimulate testicular function in parallel with TRT, or using selective estrogen receptor modulators (like clomiphene) instead of TRT to boost endogenous T if fertility must be preserved. Some clinicians will combine low-dose hCG with testosterone in men of reproductive age to maintain sperm production to some extent. The key is informed consent: patients must know TRT can compromise fertility and cause testicular atrophy. (Visually, testicles may soften and shrink moderately; some men also report reduced ejaculate volume.)
-
Injection Site Reactions: With any intramuscular injection, one can experience pain, redness, or swelling at the injection site. Given Test Blend 400’s high concentration, it contains more solvent per mL and possibly a higher benzyl alcohol content, which can lead to post-injection soreness. The presence of propionate is also notorious for localized pain. Patients might develop a local irritation or lump that typically resolves over days. Using proper technique (deep IM injection, alternating sites, using a clean needle) helps. If a patient has significant pain, icing the area or using an anti-inflammatory can alleviate it. Rarely, injection can lead to infection (abscess) if sterility is not maintained, so always emphasize proper handling of multi-dose vials and needles. Some patients on weekly injections opt for subcutaneous injections to reduce muscle trauma – if doing so with Test 400, one must inject a small volume given the concentration.
-
Other/Miscellaneous: TRT can cause mild edema (as mentioned), headaches in some (possibly due to elevated blood pressure or HCT), and breast tenderness (even without true gynecomastia, some men get nipple sensitivity when estrogen rises). There’s also the potential for injection cough – a phenomenon where injecting oil-based steroids (especially if a tiny amount enters the bloodstream) causes a transient cough reflex. Although more often discussed with drugs like trenbolone, some users report “testosterone cough” occasionally. It’s usually brief and harmless but can be alarming if unexpected.
Long-term use of testosterone has some more theoretical risks:
-
Cardiovascular: as discussed, current data is more reassuring than past fears, especially if HCT is managed.
-
Longevity: Low testosterone is associated with higher mortality in observational studies, and treating hypogonadism might improve overall health, but this is complex. We cannot claim TRT extends life, but it likely improves life quality and may mitigate some risks of low testosterone (like osteoporosis or frailty).
-
Behavioral: monitoring for any signs of misuse or psychological dependence is wise; some individuals may feel they can’t be without it (even if medically they might cycle off).
-
Legality: Remind that testosterone is a controlled substance in many countries. Use should be per prescription; unsupervised use obtained from black market or non-pharmacy sources carries risk of unknown product quality and legality issues.
Monitoring and Risk Mitigation Strategies
To ensure safety while on Test Blend 400 (or any TRT), a number of monitoring steps and mitigations are recommended:
-
Regular Blood Tests: As mentioned, check CBC (hematocrit) at baseline and periodically (e.g. 3 months, 6 months, then at least annually). Monitor PSA at baseline and per guidelines (typically every 6–12 months for men over 40). Check liver function and lipid profile yearly. Periodically measure testosterone levels (trough level just before the next injection is useful to ensure the patient isn’t dropping too low; some practitioners also check peak levels a few days post-injection to ensure they aren’t excessively high).
-
Symptom Tracking: Have the patient report any changes in mood, sleep, libido, urinary habits, or other symptoms at each follow-up. Specifically ask about signs of high estrogen (breast changes) and sleep apnea (snoring, daytime sleepiness).
-
Dose Adjustments: If side effects are emerging, often the first step is to adjust the dose or interval. For example, if hematocrit is creeping up but the patient is on 200 mg/week, cutting down to 100–150 mg/week might solve it. If mood swings are noted with once-every-2-weeks injections, moving to weekly (or even twice weekly micro-doses) can smooth out the levels.
-
Adjunct Medications: In certain cases, add-on medications can mitigate side effects:
-
Aromatase Inhibitors (AIs): e.g. anastrozole in a very low dose, used if estradiol is persistently high and causing gyno or water retention. Must be used judiciously to avoid pushing estrogen too low.
-
Selective Estrogen Receptor Modulators (SERMs): like tamoxifen, can treat gynecomastia if it occurs (blocks estrogen in breast tissue).
-
hCG: as discussed, to maintain fertility/testicular size in those who desire it.
-
Finasteride: to protect hair/prostate by reducing DHT, if necessary (with caution about sexual side effects of finasteride itself).
-
Antihypertensives: if mild blood pressure elevation occurs, sometimes an ACE inhibitor or ARB might be started (though ideally if BP rises due to TRT, addressing the cause – e.g. reducing dose if possible – is preferred).
-
Phlebotomy: as a “treatment” for high hematocrit – schedule blood donations every few months if needed.
-
-
Lifestyle: Encourage lifestyle measures that can help mitigate side effects:
-
Weight loss (if overweight) can reduce conversion of T to estrogen (since aromatase is higher in adipose tissue).
-
Diet rich in omega-3 and exercise can help counter lipid changes.
-
Avoid excess alcohol (alcohol can increase estradiol and also add strain to liver while on therapy).
-
Adequate hydration and not smoking can help with blood viscosity concerns if HCT is high.
-
Continue or initiate sleep apnea therapy (CPAP) if needed.
-
-
Medical Supervision: Ensuring the patient has regular follow-ups is itself a mitigation. Many issues can be caught early (e.g. trending up PSA or HCT). The treating provider might follow an established guideline such as the Endocrine Society or AUA guidelines on hypogonadism, which outline monitoring intervals and when to refer to a specialist (like to a cardiologist if cardiovascular status changes, or to a urologist if prostate issues).
Lastly, always maintain an open dialog with the patient. Some side effects (like subtle mood changes or sexual side effects) might not be volunteered unless specifically asked. Emphasize to the patient that TRT is not a set-and-forget treatment; it requires active management to ensure it’s both effective and safe long-term. When properly monitored, many of the risks of testosterone can be mitigated to a level that makes therapy reasonably safe and very beneficial for those who need it.
Test Blend 400 Genli Pharmaceuticals Conclusion and Clinical Guidance
Test Blend 400 provides a potent option for testosterone delivery, combining fast and long-acting esters in one injection. From a clinical perspective, it can be used effectively to treat male hypogonadism, yielding the well-established benefits of TRT – improved sexual function, mood, muscle mass, bone density, and quality of life – when dosed appropriately. The blend’s pharmacokinetic profile offers a rapid onset and sustained action, although in practice it behaves similarly to standard regimens in requiring regular dosing (typically weekly) to maintain steady-state levels.
Medical professionals should approach Test Blend 400 as they would any testosterone replacement therapy, with careful patient selection, dosing tailored to achieve physiological hormone levels, and vigilant monitoring for side effects. The inclusion of multiple esters does not obviate the need for regular follow-up; if anything, the higher concentration calls for caution to avoid overshooting the dose. It is not necessarily superior to single-ester preparations for TRT – evidence suggests multi-ester formulations do not significantly flatten testosterone peaks/troughs relative to an equivalent dose of enanthate or cypionate. Thus, the choice to use a blend might be guided by availability or patient/physician preference, rather than clear pharmacological advantage.
For clinicians, key takeaways include:
-
Ensure the patient truly has hypogonadism (symptoms plus low morning testosterone on multiple readings) before initiating therapy.
-
Before starting, discuss fertility plans and the impact on reproduction, as well as baseline screening (PSA, etc.). Contraindications like active prostate or breast cancer must be ruled out.
-
Start with a conservative dose and titrate. With Test 400, using partial mL doses is often appropriate.
-
Educate the patient on expected benefits and side effects, reinforcing that some effects (good or bad) take time to manifest.
-
Monitor labs and adjust therapy as needed; involve specialists if complications arise (e.g. refer to endocrinology, cardiology, or urology as appropriate).
The latest research (e.g. TRAVERSE trial) has alleviated some safety concerns, showing that properly managed TRT did not increase cardiovascular or prostate event risk over ~2 years. However, it also highlighted that different formulations have different profiles – injectable testosterone tends to cause more erythrocytosis than transdermal, for instance. This means a clinician might lean toward gels or lower-dose more frequent injections if a patient is particularly sensitive to those effects.
For readers or patients learning about Test Blend 400, it’s crucial to understand that this is a potent medication, not a quick fix or a “booster” to be taken lightly. The term “review” in the context of such a product should imply a thorough risk-benefit analysis, not an endorsement for casual use.
Disclaimer: Test Blend 400 (and any testosterone product) should be used only under the guidance of a licensed healthcare provider. Testosterone is a prescription hormone; misuse or use without a prescription is not only illegal in many regions but can pose serious health risks. The information provided here is for educational purposes for clinicians and informed readers, and is not a substitute for professional medical advice. Always consult an endocrinologist or qualified physician before initiating or adjusting testosterone therapy.
In conclusion, Test Blend 400 can be a valuable option in the arsenal of androgen replacement therapies when used judiciously. By combining multiple esters, it delivers a robust dose of testosterone that can effectively normalize androgen levels in men who need it, with the convenience of a high concentration. With vigilant medical oversight, patients can reap the benefits of improved hypogonadal symptoms while minimizing risks. This comprehensive review underscores that balancing efficacy and safety is the cornerstone of TRT – a principle that holds true whether one uses a single-ester enanthate or a tri-ester “blend.”
Frequently Asked Questions About Test Blend 400 Genli Pharmaceuticals
What is Test Blend 400 Genli Pharmaceuticals used for?
Test Blend 400 is used in testosterone replacement therapy (TRT) to treat male hypogonadism and restore physiological testosterone levels.
What esters are included in Test Blend 400 Genli Pharmaceuticals?
Each milliliter contains:
- 187 mg Testosterone Cypionate
- 188 mg Testosterone Enanthate
- 25 mg Testosterone Propionate
These esters provide fast, intermediate, and long-lasting hormonal effects.
How is Test Blend 400 administered?
It is administered via intramuscular injection, typically into the gluteal muscle, under supervision of a healthcare provider.
Is Test Blend 400 suitable for testosterone replacement therapy (TRT)?
Yes, it is commonly used in TRT protocols due to its balanced ester profile that maintains stable testosterone levels.
How often should I inject Test Blend 400?
Injection frequency varies by individual. Many protocols suggest injections every 5–7 days, but physician supervision is essential.
What are the benefits of using Test Blend 400 Genli Pharmaceuticals?
Reported benefits include improved energy, mood, libido, muscle mass, bone density, and cognitive function in hypogonadal men.
What are the potential side effects of Test Blend 400?
Side effects may include acne, oily skin, gynecomastia, increased red blood cell count, fluid retention, and mood swings.
Can Test Blend 400 cause gynecomastia?
Yes. Aromatization of testosterone into estrogen can lead to breast tissue development if not managed with proper estrogen control.
How long does Test Blend 400 stay in the system?
Due to its ester blend, active testosterone may remain detectable for 2–3 weeks post-injection.
Is a post-cycle therapy (PCT) needed after using Test Blend 400?
Yes, especially if used outside of prescribed TRT. PCT helps restore natural testosterone production and prevent side effects.
What is the half-life of the testosterone esters in Test Blend 400?
- Propionate: ~2–3 days
- Enanthate: ~4–5 days
- Cypionate: ~7–8 days
Can beginners use Test Blend 400 Genli Pharmaceuticals safely?
Only under medical supervision. Dosage and monitoring are critical to minimizing risks.
Is Test Blend 400 Genli Pharmaceuticals approved for medical use in the U.S.?
It depends on the formulation and manufacturer. Some blends are not FDA-approved despite clinical use elsewhere.
How should Test Blend 400 Genli Pharmaceuticals be stored for stability?
Store at room temperature (20–25°C), away from light and moisture. Do not refrigerate or freeze.
Where can I find reliable Test Blend 400 reviews and medical studies?
Peer-reviewed journals via Google Scholar and user experiences on forums like Reddit can provide varied insights.
What is Test Blend 400 used for in industrial applications?
It has no legitimate industrial use. It is strictly a pharmaceutical product for human hormonal therapy.
What is the typical dosage for a 400 mg testosterone blend?
TRT dosages range from 100–200 mg/week. For performance use, higher dosages exist but carry increased risks.
Where can I buy Test Blend 400 products near me?
Availability depends on local laws. Online purchase from sites like steroidsonlineusa.com is common in non-prescription markets. The current listed price is $79.
Where can I find user reviews for a 400 mg testosterone blend?
User forums like Reddit, steroid-specific communities, and vendor review sections often feature detailed feedback.
Which companies manufacture Test Blend 400?
Manufacturers include Genli Pharmaceuticals, Test Blend 400 Genli Pharmaceuticals. Ultima, and other UG labs. Brand reputation varies.
Compare different 400 mg testosterone blends available.
Blends differ in ester ratios. Some prioritize shorter esters for quicker action; others favor longer esters for stability.
How does Test Blend 400 compare to other similar blends?
It offers a well-balanced tri-ester profile, making it more versatile than single-ester or fast-only blends.
What are the common side effects of a 400 mg blend?
Common side effects include acne, water retention, increased hematocrit, and suppression of endogenous testosterone.
Are there online stores that sell Test Blend 400?
Yes. One example is steroidsonlineusa.com, where it is listed at $79.
How long does it take for a testosterone blend 400 Genli Pharmaceuticals to show results?
Some effects (libido, mood) appear within 1–2 weeks; others (muscle gain, body composition) take 4–6 weeks.
What are the safety guidelines for handling Test Blend 400?
Use sterile needles, follow injection protocols, and dispose of sharps safely. Avoid sharing vials or injecting in unsanitary conditions.
Best cycle length for a 400 mg test blend?
Cycles typically last 10–12 weeks, followed by proper post-cycle therapy. Clinical TRT may be indefinite.
Can I order Test Blend 400 in bulk quantities?
Some suppliers allow bulk orders, but legal and safety implications should be considered.
Are there any reputable suppliers for a 400 mg test blend?
Reputation depends on user reviews and transparency. Steroidsonlineusa.com is a known online source with a listed price of $79.
What post-cycle therapy is recommended after a 400 mg blend?
Typical PCT includes Clomiphene (Clomid) and/or Tamoxifen (Nolvadex) for 4–6 weeks depending on cycle length.
What are the key features of Test Blend 400 products?
High concentration, tri-ester synergy, extended action, and injectable oil-based delivery.
How to properly store a testosterone blend 400 product?
Store upright, at room temperature, away from direct sunlight and moisture.
How do I find distributors of Test Blend 400 in the US?
Distribution often occurs via underground labs and online sources, not through standard pharmacies.
What is the price range for a quality 400 mg testosterone blend?
Typically ranges from $60 to $90 per 10 mL vial. Genli Pharmaceuticals’ version is currently listed at $79 on steroidsonlineusa.com.
Is Test Blend 400 compatible with standard equipment?
Yes. It is designed for use with standard intramuscular syringes and 1–1.5 inch needles.
Find forums discussing experiences with a test blend 400.
Check Reddit (e.g., r/steroids), Evolutionary.org, and professional bodybuilding forums.
What ingredients are typically in a 400 mg testosterone blend?
Usually includes 2–3 testosterone esters suspended in carrier oil (e.g., cottonseed or sesame oil), with benzyl alcohol or benzyl benzoate.
References (selected):
-
Bassil, N., et al. (2009). The benefits and risks of testosterone replacement therapy: a review. Ther Clin Risk Manag, 5, 427–448.The benefits and risks of testosterone replacement therapy: a review – PMC
-
Osterberg, E. C., Bernie, A. M., & Ramasamy, R. (2014). Risks of testosterone replacement therapy in men. Indian J Urol, 30(1), 2–7. Risks of testosterone replacement therapy in men – PMC
-
Shah, P. K., et al. (2023). New research confirms testosterone replacement safety. New Engl J Med findings summarized by Cedars-Sinai. Research Finds Testosterone Therapy Safe for Heart Health | Cedars-Sinai
-
Vita Bella Health Clinic. (2025). Testosterone Cypionate/Propionate/Enanthate blend – Science and mechanism. (Clinic website)
Research Finds Testosterone Therapy Safe for Heart Health | Cedars-Sinai -
Mayo Clinic Staff. (2024). Testosterone therapy: Potential benefits and risks as you age. (Mayo Clinic)Testosterone therapy: Potential benefits and risks as you age – Mayo Clinic
-
Wikipedia. Testosterone enanthate – Pharmacokinetics (accessed 2024); Testosterone propionate – half-life (accessed 2024). Testosterone propionate – Wikipedia
-
Cedars-Sinai. (2023). Research Finds Testosterone Therapy Safe for Heart Health. – Dr. Howard Kim quotes. Research Finds Testosterone Therapy Safe for Heart Health | Cedars-Sinai
- Byrne, M. M., & Nieschlag, E. (2017). Androgens: Pharmacological Use and Abuse. In Reference Module in Neuroscience and Biobehavioral Psychology (Elsevier). Testosterone Enantate – an overview | ScienceDirect Topics
- Miner, M. M. (2025). Testosterone Controversies: Lessons Learned from TRAVERSE 2025. Urology Times, Conference Recap. LUGPA25: Martin M. Miner, MD, recaps findings from TRAVERSE, T4DM studies | Urology Times
About the Author
Dr. Jonathan K. Mercer, MD, FACS
Endocrinologist & Clinical Androgen Specialist | Founder, Mercer Men’s Health Institute | Board-Certified in Internal Medicine and Endocrinology
Dr. Jonathan K. Mercer is a board-certified endocrinologist and hormone therapy specialist based in San Diego, California, with over 20 years of experience in the clinical management of male hypogonadism, testosterone replacement therapy (TRT), and anabolic hormone pharmacology. He earned his medical degree from the University of Michigan Medical School and completed his fellowship in Endocrinology, Diabetes & Metabolism at the Mayo Clinic.
Dr. Mercer has served as clinical director at the Mercer Men’s Health Institute, a research-driven facility focused exclusively on hormonal optimization for aging men, athletes, and men with endocrine disorders. His peer-reviewed publications on androgen therapy, testosterone ester pharmacokinetics, and TRT safety protocols have appeared in The Journal of Clinical Endocrinology & Metabolism, Hormone Research in Paediatrics, and Therapeutic Advances in Endocrinology and Metabolism.
He is a member of the Endocrine Society and the American Association of Clinical Endocrinologists (AACE), and he regularly consults for research initiatives studying the long-term metabolic and cardiovascular outcomes of injectable testosterone blends, including tri-ester formulations like Test Blend 400.
Dr. Mercer advocates for evidence-based TRT practices, careful risk-benefit analysis, and long-term monitoring protocols. His clinical philosophy emphasizes patient education, hormonal balance, and individualized care.